GENERAL MEDICINE CASE DISCUSSION
FINAL PRACTICAL :SHORT CASE
This is an E log book to discuss our patient's de-identified health data shared after taking his guardian's signed informed consent. Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable comments in comment box are most welcomed
I have been given this case to solve in an attempt to understand the topic of "Patient clinical data analysis" to develop my competency i reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
K.TEJARSHINI
HALL TICKET No:1701006083
June,08,2022.
CASE DISCUSSION:
A 65Year old female known case of chronic kidney disease (CKD) with multiple hemodialysis (MHD)came to the hospital for dialysis with chief complaints of,
Fever,dysuria,burning micturition.
HISTORY OF PRESENTING ILLNESS:
She was apparently asymptomatic 13 years back, In the year 2011 (7/2/11)she complained of fever ,lower back ache and burning micturition for which they went to hospital and USG was done (small b/l kidneys) with serum creatinine of value 2.0 .
From 2012 to 2018 occasional recurrent UTI.
On 21/05/22 complained of leg swelling, decreased appetite,nausea ,vomiting for which they consult nephrologist Diagnosed CKD +UTI+UROSEPSIS with ANAEMIA where she was on dialysis (done 4 dialysis outside hospitals)+AV FISTULA on 27/05/2022.
In our hospital 2 dialysis were done.
TIME LINE OF EVENTS:

PAST HISTORY:
Known case of CKD since 13years and on medical management.
Known case of osteoarthritis,L5-6/L5-S1 RADICULOPATHY diagnosed on 9/08/22 for which she used NSAIDS for 1year.
Not a known case of HTN,THYROID,CAD, DIABETES,CVA,TB, EPILEPSY.
PERSONAL HISTORY:
Appetite:Decreased
Diet:Mixed (stopped eating red meat past 10 years)
Bowel habits:Regular
Bladder habits: Burning micturition
Sleep:Adequate
No Addictions.
FAMILY HISTORY:
No similar complaints in the family.
GENERAL EXAMINATION:

INVESTIGATIONS:
2/06/2022:
RBS:74mg/dl
7/06/2022:
RFT:
Urea:84mg/dl
Creatinine:4.1mg/dl
Uric acid:4.3mg/dl
Calcium:9.5mg/dl, phosphorus:4.2mg/dl,Sodium:142mEq/L, Potassium:3.6mEq/L,chloride:102mEq/L
8/06/2022:
COMPLETE BLOOD PICTURE (CBP):
Hb:8.9 gm/dl
Total count:6,400 cells/cumm
Neutrophils:75%,Lymphocytes:20%, Eosinophils:1%, Monocytes:4%, Basophils:00,Platelet count:1.20lakhs/cumm.
SMEAR: Normocytic Normochromic Anemia with thrombocytopenia.
ABG:
PH:7.50
PCO2:31.7mmHg,PO2:141mmHg,
HCO3:24.6mmol/L,St.HCO3:26.2mmol/L,
BEB:2.0mmol/L,BEecf:1.6mmol/L,TCO2:51 VOL,
O2 sat:98.8%,O2 Count:12.6vol%.
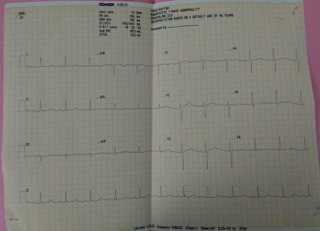
ECG:

TREATMENT:
7/06/2022 ,9PM:
Inj.LASIX 40mg/Po/BD(if SBP >110mmHg)
TAB.NODOSIS 500mg/Po/BD
TAB.OROFEX-XT/Po/OD
TAB.SHELCAL 500mg/Po/OD
CAP.BIO-D3/Po/OD
Inj.NORADRENALINE-DS@5ml/hr(increase or decrease according to MAP)
8/06/2022:
TAB.LASIX 40mg/Po/BD(ifSBP>110mmHg)
TAB.ECOSPRAN 75mg/Po/OD
Inj.IRON SUCROSE once weekly
Inj.RENOCEL twice weekly
TAB.PAN 40mg/Po/OD
TAB. SHELCAL 500mg/Po/OD
Inj.Noradrenaline- DS 5ml/hr(increase or decrease according to MAP)

Comments
Post a Comment