General medicine case discussion
Date: 11/03/2022
This is is an online E log book to discuss our patient's deidentified health data shared after taking his/her/guardian's signed in formed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence-based inputs.This e-log book also reflects my patient centered online learning protfolio and your valuable inputs on comment box is welcome.
Roll no : 61
2017 Batch
I''ve been given this case to solve in an attempt to understand the topic of "PATIENT CLINICAL DATA ANALYSIS" to develop my competency in reading and comprehending clinical data including history,clinical findings,investigations and comeup with Diagnosis and Treatment plan.
A 70year old female resident of narketpally came to the hospital with complaint of fever from 4 days.
Date of admission:10/03/2022
History of present illness:
Patient was apparently symptomatic 20days back then she complained of fever which is insidious in onset ,highgrade intermittent type of fever associated with chills and rigor,relieved on medication and again it appears and she mentioned that whenever she eats food fever returns.
She visited our hospital and blood test were done and prescribed medication and fever get relieved.
Since 4days she again complained of fever which is highgrade, intermittent type associated with chills and rigor,no evening rise of temperature aggravated on eating food, relieved upon medication (2tabs.perday of paracetamol).
Then she visited a local hospital there her BP checked and doctor confirmed that she is hypertensive and prescribed medication and she taken the tablets and tablet sheet prescribed by doctor were completed and she is not taking the tablets.
Doctor prescribed medication for control of fever but fever appears again after discontinuation of medication and he suggested to visit our hospital (in think of malaria,dengue)
She also complained of slight headache during fever attack.
No history of cough,cold,myalgia,weight loss,sore throat.
No history of pain abdomen , constipation,vomitings.
No history of joint pains,epistaxis,retro orbital pain.
No history of burning micturition,increased or decreased frequency of urine.
No history of palpitations,fatiguability,shortness of breath.
Past history:
Not a K/C/O of DM,TB,Epilepsy.
No history of blood transfusion.
History of left eye surgery for pterygium.
Personal history:
Appetite:Normal
Diet:Mixed
Sleep: Adequate
Bowel and bladder habits:Regular
No Addictions.
Family history:Insignificant
General Examination:
Conscious, coherent, co-operative
Moderately built and nourished.








Systemic Examination:
CNS EXAMINATION:
Higher mental functions intact
Cranial nerve ,sensory,motor system examination:normal
Provisional diagnosis:
Fever under evaluation with AKI
Investigations:
14/02/2022:
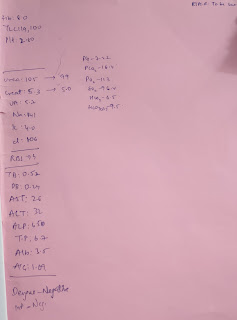
Hemogram:

LFT:


Serum electrolytes:

ESR:

Blood parasite:

ECG:

Chest x-ray:

11/03/2022:
Chest x-ray:

USG:

Color Doppler 2D Echo:

ECG:






Treatment:
10/03/22:
IVF NS ,RL @100ml/hr
Inj.PAN 40mg I.V/OD
Temp charting 4th hourly
Inj .OPTINEURIN 1amp in 100ml NS I.V/OD
Inj NEOMOL 1gm I.V SOS(if temp >101°F)
Tab.DOLO 650mg PO/TID
Inj.MONOCEF 1gm I.V BD
11/03/2022:
IVF NS,RL @50ml/hr;DNS @100ml/hr
Inj MONOCEF 1gm I.V BD
Inj PAN 40mg I.V/OD
Inj.OPTINEURIN 1amp in 100ml NS I.V/OD
Strictly I/O charting
12/03/2022:
O/E:
BP:130/70mmof hg ,RR:24cycles/min,pulse rate:79bpm
IVF NS,RL @50ml/hr
Inj.PIPTAZ 2.25gms I.V TID
Inj OPTINEURIN 1amp in 100ml NS I.V/OD
Strictly I/O charting
Inj.PAN 40mg I.V/OD
Temp charting 4th hourly
Tab.DOLO 650mg PO SOS
Inj.NEOMOL 1gm I.V SOS
Tab.DOXY 100mg PO BD
Plenty of oral fluids
Tab. NODOSIS 500mg PO TID
BP,Pulse rate 4th hourly monitoring
13/03/2022:
IVF NS,RL @50ml/hr
Inj. PIPTAZ 2.25gms I.V TID
Inj OPTINEURIN 1amp in 100ml NS I.V/OD


Comments
Post a Comment